Pancreatic Insufficiency
Digestive enzymes are produced in the pancreas and secreted into the gut to help breakdown food and release the nutrients which can then be absorbed into the bloodstream.
Pancreatic insufficiency is the reduction of production or transportation of the digestive enzymes, which results in the inability to properly digest a meal (fats, proteins and carbohydrates). The insufficiency is not absolute, it is variable, which then has a graded impact on digestion and hence symptoms. Patients can suffer from a variety of gastric symptoms, ranging in severity, but including abdominal pain, weight loss, diarrhoea, smelly loose stools, flatulence, loss of appetite and fatigue. All of these can be confused with symptoms of a variety of other gastric complaints. Hence, performing a simple stool test to determine the level of elastase (a pancreatic enzyme), helps with the diagnosis of this condition. Clinicians then just need to determine the cause…
Pancreatic insufficiency really is just another symptom but the cause is almost always pathogenic, resulting from conditions such as chronic pancreatitis, cystic fibrosis, diabetes mellitus, Crohn’s disease, pancreatic cancer plus a variety of other things including lifestyle choices and ageing.
Historically assessment of pancreatic function has been carried out using invasive, unpleasant and expensive procedures including colonoscopy, Secretin Stimulation test, CT and Endoscopic Retrograde Cholangiopancreatography (ERCP). Pancreatic elastase doesn’t undergo any significant degradation during the digestive transit and is fairly stable in stool samples, so the levels are used as a marker to determine pancreatic activity as a whole.
Measurement of faecal elastase has been shown to be an excellent practical and cost-efficient alternative to these historic invasive procedures to determine the level of pancreatic function, although it must be performed using a formed stool. Liquid stools will almost inevitably lead to a falsely low reading due to the additional water content diluting out the elastase. Having an extremely high negative predictive value of ~99% is valuable in helping to determine the cause of variable gastric symptoms.
Testing Pancreatic Elastase
The new BÜHLMANN fPELA assay utilises the same CALEX extraction device as the fCAL turbo assay, so it is possible to run both tests from a single extract.
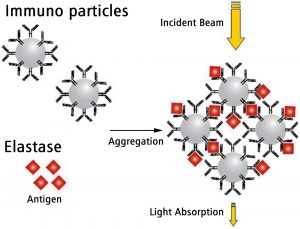
The fPELA assay is random access and runs on standard clinical chemistry analysers (Roche, Abbott, Beckman, Siemens etc) although there is also a stand-alone solution as well. The assay is turbidimetric, with a dynamic range of 10 – 5000μg/g. Time to first result is 10 minutes with further results following every few seconds thereafter, making it one of the fastest faecal elastase assays available.
As with all faecal elastase assays it is recommended not to test using liquid samples because the additional fluid will dilute out the elastase giving a falsely low result.
Data from historic NEQAS samples shows the new BÜHLMANN fPELA gives comparable results to the current ELISA based methods:


 BÜHLMANN fPELA Assay For Faecal Pancreatic Elastase
BÜHLMANN fPELA Assay For Faecal Pancreatic Elastase








